

- Sustainability
- DE&I
- Pandemic
- Finance
- Legal
- Technology
- Regulatory
- Global
- Pricing
- Strategy
- R&D/Clinical Trials
- Opinion
- Executive Roundtable
- Sales & Marketing
- Executive Profiles
- Leadership
- Market Access
- Patient Engagement
- Supply Chain
- Industry Trends
Payer Perspectives on Gene Therapy Reimbursement
Pharmaceutical Executive
A follow-up survey of clinical and financial health plan leaders uncovers evolving approaches and views on the management of high-cost, curative-intended treatments with one-time administration.
The reimbursement of emerging durable and potentially curative cell and gene therapies challenge US payers due to their high upfront costs. In addition, the lack of long-term clinical durability data amplifies uncertainties that complicate payer coverage and reimbursement determinations. These cell and gene therapy characteristics could negatively impact patient access and, ultimately, future developer innovation.
The Financing and Reimbursement of Cures in the US (FoCUS) project was launched in 2016 by MIT’s NEWDIGS Initiative with the objective of elucidating the challenges and financial impact created by durable/potentially curative therapies and providing implementable models to manage the financial impact on the US healthcare system. To that end, FoCUS has conducted two surveys to reveal present payer perspectives regarding current and future management of high-cost durable therapies with one-time administration.
The first FoCUS payer survey (FOCUS I) was conducted in August to September 2017 as the initial chimeric antigen receptor (CAR) T-cell therapies, Kymriah (tisagenlecleucel/Novartis) and Yescarta (axicabtagene ciloleucel/Kite Pharma) were being approved. It consisted of structured telephone interviews with 15 payers across multiple payer segments.1,2 At that time, payers had variable awareness and readiness to manage the new cost of these and other emerging gene therapies such as Luxturna (voretigene neparvovec-rzyl/Spark Therapeutics), which was approved in December 2017. One-third of these payers were newly aware and learning about these therapies, with 40% watchfully waiting and 27% engaged in active management. Payers were open to financing mechanisms, with 47% expressing a willingness to engage in innovative financing models, performance-based annuities, and risk-pooling.
Additional payer surveys were published by the Alliance for Regenerative Medicine (ARM) and the National Association of Managed Care Physicians (NAMCP) of 36 respondents in March to June 20173 and the National Pharmaceutical Council (NPC) of 21 respondents in February to March 2018.4 While specific questions and methodologies differed, in combination, the three surveys reported a general progression in awareness and concern regarding management of durable therapies, with 10% (ARM/NAMCP) to 27% (FOCUS I) and, ultimately, 100% of payers (NPC) reporting having started to consider coverage or operational issues associated with these treatments.
The most recent FoCUS payer survey (FOCUS II), consisting of 15 online questions, was conducted with clinical and financial health plan leaders from 77 US payers between September 2018 and April 2019 (note: Novartis gene therapy Zolgensma was approved in the US in May 2019 and launched two months later). The survey again focused on assessing payer perspectives regarding current and future management of high-cost durable, potentially curative therapies with one-time administration.
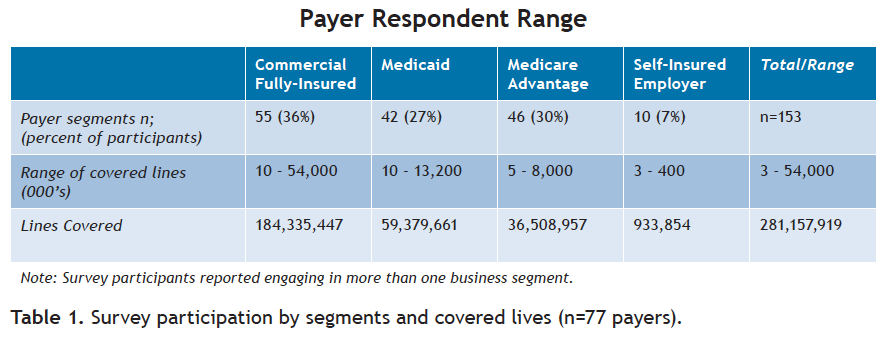
Participants in the FOCUS II survey represented 153 payer segments, including commercial fully-insured plans, self-insured employers, Medicare, and Medicaid. Payers ranged in size from less than 5,000 insured lives to upwards of 50 million and in total covered over 280 million lives (see Table 1).


Click to enlarge
The survey did not control for more than one person from the same plan completing the survey. Results from intermediaries such as pharmacy benefit managers were excluded to the extent they could be identified.
Respondents self-identified among roles in pharmacy (53%); medical (31%); human resources and benefits (9%); and finance and actuary (7%).
Three major findings from FOCUS II
1) While payers are concerned about financial risk and impact of high-cost durable therapies, nearly all are covering them
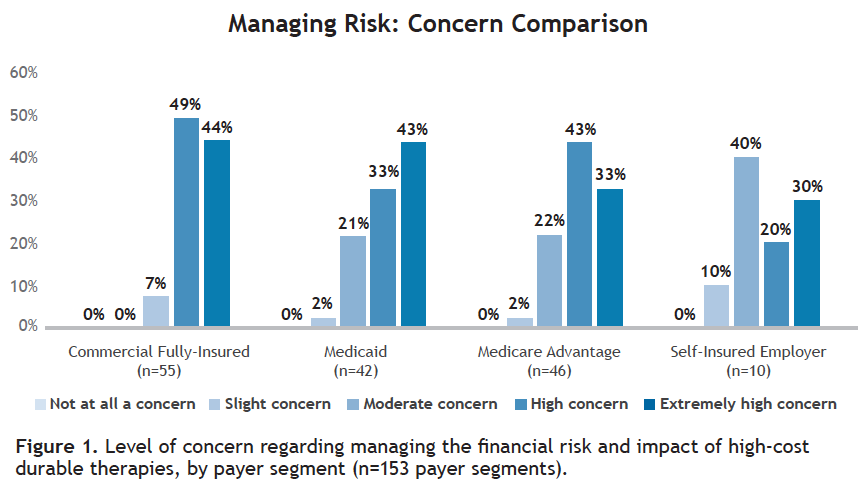
All payers have some level of concern related to the financial risk and impact of these treatments. Eighty percent of payers rate their concern as high or extremely high, with 39% of 153 payer segments rating their concern as extremely high, 41% as high, 18% as moderate concern, 2% as slight concern, and 0% as no concern.
When analyzed by payer segment, commercial fully-insured plans expressed the highest levels of concern, with 93% reporting a high or extremely high concern and 7% reporting a moderate concern (see Figure 1). In comparison, only 50% of self-insured employers reported a high or extremely high concern, with other payer segments in-between, with 76% reporting high or extremely high concern.


Click to enlarge
Payers selected a number of reasons for their high or extremely high concern:
- The total cost is material for the plan (98%).
- Drug performance risk (effectiveness and durability) (91%).
- Actuarial risk (likelihood of encountering an orphan case) (91%).
- Payment timing relative to benefit realization (offsets may not cover the high cost of treatment) (84%).
Other identified reasons for high concern include:
- Burden of multiple high-cost therapies.
- Concern about what this will represent in three to five years with respect to total cost.
- Potential off-label use.
- Operational management of a larger pipeline.
- Adverse selection.
Nearly all payers surveyed (99%) currently covered one-time, high-cost durable therapies; 46% cover all treatments then approved, while 53% cover some. For those covering high-cost durable therapies, payers are evenly divided regarding utilization management practices. Forty-eight percent cover high-cost durable therapies as specified in the FDA-approved label. Forty-nine percent apply utilization management coverage with more restrictions than the FDA-approved label. Three percent cover with less restrictions than the label.
Commercial fully-insured payers are the most restrictive, with 62% managing coverage with more restrictions than the FDA-approved label. Fifty-four percent of Medicaid plans reported utilization management that was more restrictive than the label, with 44% covering as specified in the label. Medicare Advantage is the least restrictive, with 67% managing consistent with the label and 31% more restrictive.
Case management is used by 82% of payers and centers of excellence (COE) are required for 64% of payers surveyed. Thirty percent restrict use of all high-cost durable treatments to COE, while 34% restrict some of these treatments to COE.
2) Payers are motivated to manage the financial risk associated with durable one-time treatments differently, making this a high priority over the next two years
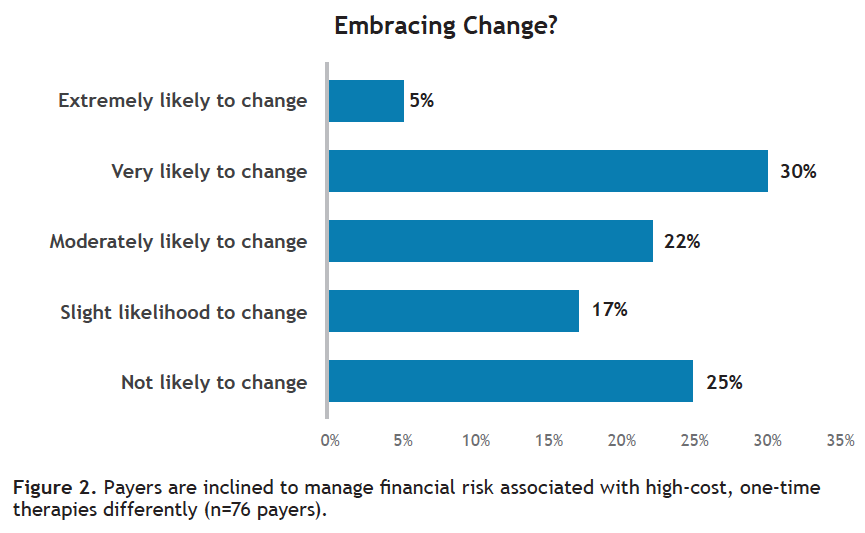
In contrast to high-cost chronic treatments such as Spinraza (nusinersen/Biogen) or Onpattro (patisiran/Alnylam Pharmaceuticals), the majority of payers reported they were moderately, very, or extremely likely to change how they manage the financial risk associated with one-time, high-cost durable treatments (see Figure 2).


Click to enlarge
Payers were somewhat mixed regarding the importance of high upfront cost per patient and cumulative per member per month (PMPM) to their organization’s serious consideration of alternative approaches to manage financial risk of one-time, high-cost treatments. Thirty-nine percent rated both factors as equal. Thirty-one percent reported that high upfront therapy cost per patient is much or somewhat more important, while 26% reported that high total PMPM impact is much or somewhat more important. Neither factor would trigger serious consideration of an alternative payment model for 5% of those surveyed.
Implementing new management strategies for these therapies is a near-term objective. Fifty-seven percent of 77 payers surveyed expect to implement a new management strategy in the next one to two years, while 13% already have. Figuring out the best way to finance new high-cost durable therapies is a high or very high priority for 76% of payers surveyed, a medium priority for 21%, and a low priority for 4%.
New strategies that payers reported have already been implemented included value-based or outcome-based agreements and changes in provider contracting, including carving out payment for these treatments to a third party such as reinsurance or risk pools and global case rate payments.
Payers expressed interest in multiple financing approaches for the future. Overall, payers were most interested in short-term milestone-based contracts, defined as contracts of less than two years duration where the therapy is paid for upfront and the plan receives refunds tied to performance (see Table 2).


Click to enlarge
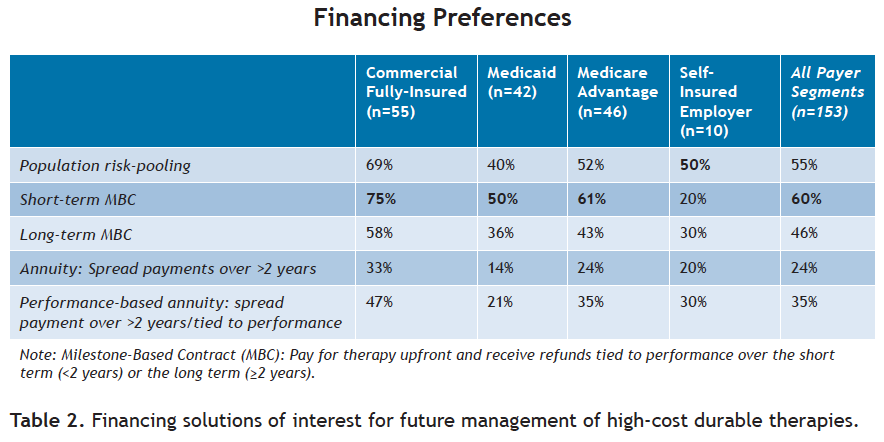
Self-insured employers were most interested in population risk-pooling, stop-loss/reinsurance over the broader population. Installment payments, annuities without a performance component, were the least appealing, with only one-third of commercial plans to a low of one-seventh (14%) of Medicaid respondents expressing interest.
3) Addressing contract terms and barriers will matter
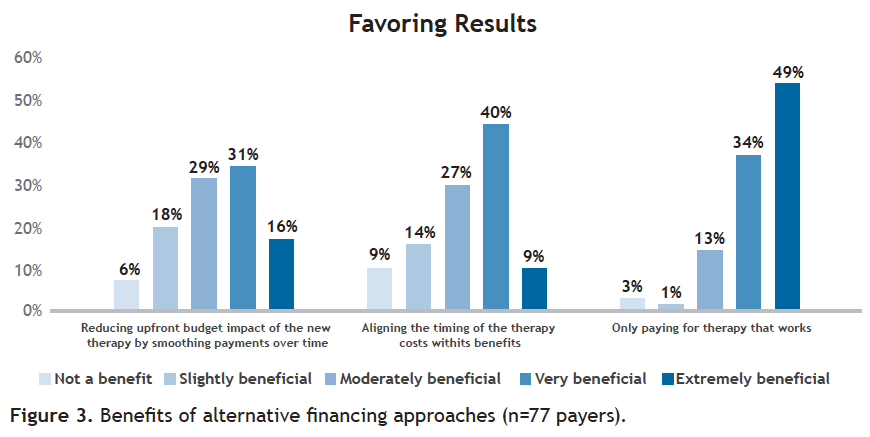
Payers see multiple benefits of alternative financing approaches:
- Reducing upfront budget impact of the new therapy by smoothing payments over time.
- Aligning the timing of the therapy costs with its benefits.
- Only paying for therapy that works by including performance-based requirements for initial or continued payment.
Of the three, payers see the most benefit in paying for what works, with 83% identifying this factor as extremely or very beneficial (see Figure 3).


Click to enlarge
The majority of payers identified a number of elements of multi-year, performance-based agreements as very important or a deal-breaker. These include:
- The inclusion of performance-based requirements for payment (72%).
- Termination of payment obligation with the death of the patient (67%).
- Access to data on specific measures (66%).
- Term: The number of years over which the payouts are stretched (65%).
- Ability to track performance even if the patient has left the plan (62%).
Finally, payers rated a number of barriers to alternative financing approaches (see Figure 4). Using the two top levels of importance-extremely important and very important-payers identified operational, strategic, and structural barriers.


Click to enlarge
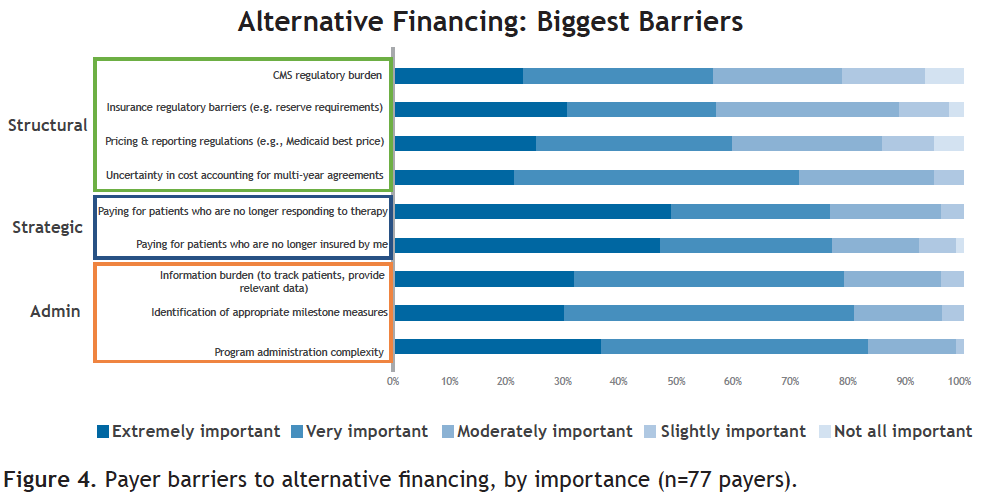
The top-rated operational barriers reported were:
- Program administration complexity (83%).
- Identification of appropriate milestone measures (81%).
- Information burden for tracking patients and providing relevant data (79%).
The top-rated strategic barriers were:
- Paying for patients who are no longer insured by the plan (77%).
- Paying for patients who are no longer responding to therapy (76%).
The top rated structural barriers were:
- Uncertainty in cost accounting for multi-year agreements (71%).
- Pricing and reporting regulations (e.g., Medicaid best price) (59%).
- Insurance regulatory barriers (e.g., minimum reserve requirements) (57%).
- CMS regulatory burden (56%).
Implications
The FOCUS II survey shows payers awareness and concerns have grown since FOCUS I in 2017 regarding the impact of high-cost durable, potentially curative therapies with one-time administration. Compared with the prior FoCUS survey and the 2017 ARM/NAMCP survey that reported just over 10% of medical directors had started to consider coverage or operational issues associated with these treatments,3 payers now have a sense of urgency. This level of concern has increased over time as more treatments have entered the market and clarity regarding the pipeline and likely approvals over time has grown.5,6
Payer concerns were consistent with the financing challenges FoCUS has previously identified,7 namely actuarial risk, therapeutic performance risk, and payment timing relative to benefit gained. In addition, payers emphasized the impact of the total cost of treatment, both for an individual patient and the burden of multiple high-cost therapies.
As a result, payers have already started to manage these treatments using many of the current management strategies they currently employ for other high-cost treatments.
And payers are interested in managing the financial risk and impact associated with these one-time curative therapies differently. Payers are open to multiple different approaches, although most favor short-term milestone-based contracts where therapy is paid for upfront and potential refunds are tied to failure to achieve performance metrics over the first two years following treatment.
This focus on a short-term, performance-based approach is consistent with payers’ emphasis on paying for what works balanced with the administrative complexities of tracking patients for measurement over time and the increased risk over time that the patient may no longer be enrolled in the plan. Addressing these and other barriers will increase the likelihood of payers adopting more advanced financing solutions.
Implementation of new management approaches is on the short-term horizon for the majority of payers and is a high priority. Both factors increase the likelihood that action will be taken.
Those actions will face a number of barriers. Payers will need to work through administrative issues and strategic positioning to facilitate alternative financing approaches. Of somewhat less importance to the plan, but high interest to other stakeholders, are issues related to regulation. Flexibility in current price reporting, such as Medicaid best price, and other insurance regulatory and accounting requirements will need to be addressed at a structural, systems level to enable implementation of these innovative models.
Jane Barlow is senior advisor to the FoCUS Project and Chief Clinical Officer for Real Endpoints; Matt Courtney is communications assistant to the FoCUS Project and Graduate Research Assistant at Harvard University; and Mark Trusheim is strategic director, NEWDIGS, and visiting scientist, Sloan School of Management, Massachusetts Institute of Technology.
The authors would like to acknowledge the Huron Consulting Group for their in-kind consulting services and honoraria to support this payer survey.
References
1. Barlow JF, Yang M, & Teagarden R. Are payers ready, willing, and able to provide access to new durable gene therapies? Value Health. 2019;22(6):642-647. https://doi.org/10.1016/j.jval.2018.12.004. Accessed June 11, 2019.
2. MIT NEWDIGS FoCUS Project. Payers open to innovative financing mechanisms for high cost gene therapies.
http://newdigs.mit.edu/sites/default/files/FoCUS%20R esearch%20Brief_2017F212-012.pdf. Published December 15, 2017. Accessed June 11, 2019.
3. Faulkner E, Werner M, Slocomb T, Han D. Ensuring patient access to regenerative and advanced therapies in managed care: how do we get there? ARM Monograph 2018 Journal of Managed Care Medicine.https://alliancerm.org/wp-content/uploads/2018/05/JMCMArm.pdf. Accessed June 11, 2019.
4. Ciarametaro M, Long G, Johnson M, Kirson N, Dubois R. Are Payers Ready To Address The Financial Challenges Associated With Gene Therapy? Health Affairs Blog. doi: 10.1377/hblog20180626.330036. Published June 28, 2018. Accessed June 11, 2019.
5. Quinn C, Young C, Thomas J, Trusheim M. Estimating the clinical pipeline of cell and gene therapies and their potential economic impact on the US healthcare system. Value Health. 2019;22(6):621-626. https://doi.org/10.1016/j.jval.2019.03.014. Accessed June 11, 2019.
6. MIT NEWDIGS FoCUS Project. Projections from the existing pipeline of cell and gene therapies.
https://newdigs.mit.edu/sites/default/files/FoCUS%20Research%20Brief%202018F210v027.pdf. Published October 29, 2018. Accessed June 11, 2019.
7. MIT NEWDIGS FoCUS Project. Precision financing solutions for durable / potentially curative therapies.
https://newdigs.mit.edu/sites/default/files/MIT%20FoCUS%20Precision%20Financing%202019F201v023.pdf. Published January 24, 2019. Accessed June 11, 2019.
















Fierce Females in the Life Science Space
March 29th 2024In this week’s episode, in recognition of international women’s month, Editor Miranda Schmalfuhs has compiled audio clips from interviews with female KOLs that she's been fortunate enough to speak with over this past month for content across a few of our brands.





